
 Test")
Borderline Personality Disorder (BPD) Test
A Clinician-Written Self-Reflection Guide Based on DSM-5 Criteria
By Kelly Pinnick, DBT-Linehan Board of Certification, Certified Clinician | Southside DBT | Telehealth across Georgia
| Important: This guide is a clinician-written educational resource, not a diagnostic tool. Only a licensed mental health professional can diagnose BPD. The self-reflection questions in this guide are based on DSM-5 criteria and are designed to help you identify patterns worth discussing with a professional. They are not a substitute for clinical assessment. |
If you are reading this, you are probably doing something that takes real courage: looking honestly at your own patterns and wondering if they have a name.
Maybe you have been told by people who love you that your emotions are too intense, your reactions too extreme, your relationships too volatile. Maybe you have spent years feeling like you are fundamentally different from other people in ways you cannot explain. Maybe you found the term Borderline Personality Disorder somewhere and felt an unsettling recognition.
Or maybe you have been given a BPD diagnosis and are trying to understand what it actually means beyond the clinical language.
This guide is written for all of those situations. It will explain what BPD is at the clinical and human level, walk you through all nine DSM-5 diagnostic criteria with specific self-reflection questions, address the most common misunderstandings and misdiagnoses, and tell you clearly what happens next, including why DBT is the most evidence-supported treatment for BPD and what that treatment actually looks like.
This is not a button you click to get a score. It is a thorough, honest, clinician-written resource that respects your intelligence and your experience.
Part 1: What Is Borderline Personality Disorder?

Borderline Personality Disorder is a mental health condition characterized by a pervasive pattern of instability in interpersonal relationships, self-image, and emotional experience, combined with marked impulsivity. This pattern typically begins in early adulthood and is present across a variety of contexts.
That is the clinical description. Here is the human one.
BPD is the experience of having an emotional system that operates at higher intensity and with less natural regulation than most people’s. It is the experience of caring deeply about relationships and simultaneously fearing, often with certainty, that the people you care about will leave or reject you. It is the experience of not having a stable, consistent sense of who you are. It is the experience of impulsive urges that feel impossible to resist in the moment. And it is the experience of behaving in ways that you later regret and cannot fully explain, because the emotional state that drove those behaviors has passed and left something like wreckage behind.
BPD is not a character flaw. It is not a choice. It is not evidence that someone is bad, manipulative, or untreatable. It is a condition with clear developmental and neurobiological roots, and it is one of the conditions for which the most robust evidence-based treatment, DBT, was specifically developed.
How Common Is BPD?
Estimates suggest that BPD affects approximately 1.6 to 5.9 percent of the general population, making it one of the more common personality disorders. It is significantly more common in clinical settings, where rates of 10 to 20 percent among psychiatric outpatients and up to 20 percent among inpatients have been reported.
Despite its prevalence, BPD remains one of the most misunderstood, most stigmatized, and most frequently misdiagnosed conditions in mental health. People with BPD have often spent years receiving other diagnoses, or receiving no diagnosis at all, before BPD is identified.
| BPD was originally developed as a diagnosis in the late 1970s. The name itself is now considered by many clinicians to be poorly descriptive. Marsha Linehan, who created DBT specifically for BPD, has proposed that the condition be renamed Emotion Dysregulation Disorder, which more accurately describes what the condition actually involves. |
Part 2: The Nine DSM-5 Criteria — With Self-Reflection Questions
A BPD diagnosis requires meeting at least five of the nine criteria listed in the DSM-5. The following section presents each criterion, explains what it means in practical human terms, and provides self-reflection questions that can help you identify whether a given pattern applies to your experience.
Read each section carefully and honestly. There are no right or wrong answers. The goal is self-knowledge, not a score.
| How to Use This Section | For each criterion, reflect on whether the described pattern is present in your life in a way that is persistent, has been present across different relationships and situations, and began in early adulthood or adolescence. Occasional experiences of these things are universal. The BPD pattern is one of pervasive, consistent presence across your life. |
| Criterion 1: Frantic Efforts to Avoid Abandonment |
| Do you experience intense fear of being left or rejected, even when others have not indicated they plan to leave? Do you take extreme measures to prevent real or imagined abandonment? |
| This criterion refers not to reasonable concern about ending relationships, but to a profound, often desperate fear of abandonment that is disproportionate to the situation. People with this pattern may read neutral actions as evidence of rejection, may repeatedly seek reassurance that is never fully satisfying, may react with intense panic or rage to perceived distance or criticism, or may take dramatic action to prevent someone from leaving even when leaving was not actually being considered. The fear is the defining feature, not the reality of the threat. |
| Criterion 2: Unstable and Intense Interpersonal Relationships |
| Do your significant relationships tend to alternate between extreme idealization and extreme devaluation? Do you go from feeling that someone is the most wonderful person in your life to feeling they are terrible, with little middle ground? |
| This pattern is sometimes called splitting: the tendency to experience people as all good or all bad, often shifting between these poles rapidly and in response to relatively small events. The person may be placed on a pedestal following the beginning of a relationship or a gesture of care, and then experienced as entirely negative following a perceived disappointment or slight. The intensity of both the idealization and the devaluation is characteristic. People with this pattern often describe relationships that feel extraordinarily close and then catastrophically destroyed, repeatedly. |
| Criterion 3: Identity Disturbance |
| Do you have an unstable or unclear sense of who you are? Does your self-image, values, goals, or sense of identity shift dramatically or feel absent or hollow? |
| Identity disturbance in BPD is more than normal self-questioning or personal growth. It is the experience of not having a stable core sense of self to return to. A person’s values, sexual identity, career goals, beliefs, and fundamental preferences about themselves may shift dramatically, sometimes in response to the people around them. Some people describe it as feeling like they take on whoever they are with. Others describe a persistent emptiness where a self should be, or a sense that they are performing a version of a person without a genuine self underneath. |
| Criterion 4: Impulsivity in Potentially Self-Damaging Areas |
| Do you engage in impulsive behaviors in at least two areas that could be harmful to you, such as spending, substance use, reckless driving, binge eating, or risky sexual behavior? |
| This criterion refers to impulsivity that is self-damaging, not simply spontaneous. The person acts on urges with little consideration of consequences, often in the context of emotional distress. The behavior provides immediate relief or stimulation but carries significant costs. What distinguishes this from ordinary impulsivity is both the consistency of the pattern across time and the degree to which the person recognizes the behavior as problematic while feeling unable to stop it. |
| Criterion 5: Recurrent Suicidal Behavior, Gestures, or Threats, or Self-Harming Behavior |
| Have you repeatedly engaged in suicidal behavior, made suicidal gestures or threats, or engaged in self-harming behaviors such as cutting or burning? |
| This is one of the most serious criteria and one that requires honest reflection without minimization or alarm. Self-harm in BPD frequently serves a regulatory function: it provides relief from unbearable emotional states, breaks through emotional numbness, or provides a sense of control. Suicidal behavior may occur in the context of acute emotional crises and may be communicated to others. It is important to note that the presence of this criterion does not make a person untreatable or hopeless. DBT was specifically developed to reduce suicidal and self-harming behaviors, and it has the strongest research evidence of any treatment for exactly this presentation. |
| If you are currently experiencing thoughts of suicide or self-harm, please reach out now. Call or text 988, or text HELLO to 741741. You do not need to manage this alone. |
| Criterion 6: Emotional Instability Due to Marked Reactivity of Mood |
| Do you experience intense mood episodes, such as intense irritability, anxiety, or dysphoria, that typically last a few hours and rarely more than a few days, often in response to interpersonal situations? |
| The mood instability in BPD is distinct from the mood cycling in bipolar disorder in several important ways. BPD mood states are typically brief, lasting hours rather than days or weeks, are highly reactive to interpersonal events, and return to baseline relatively quickly. The person may experience extreme anger, despair, or anxiety in response to perceived slights, rejections, or disappointments, with the intensity of the reaction seeming disproportionate to the trigger. Between these episodes, the person may feel relatively stable, which is different from the sustained mood states characteristic of bipolar disorder. |
| Criterion 7: Chronic Feelings of Emptiness |
| Do you experience a persistent, chronic sense of emptiness or boredom? Does life often feel hollow or meaningless even in the absence of acute distress? |
| Chronic emptiness is one of the most consistently reported experiences of people with BPD and one of the least discussed in public descriptions of the condition. It is not sadness or depression, though it may accompany both. It is more accurately described as a felt absence, a hollowness, a sense that something fundamental is missing from experience. People often describe it as a void or a feeling of not being real. This emptiness is one reason that intense experiences, including intense conflict and self-harm, can feel temporarily relieving: they break through the numbness of the emptiness and provide a sense of being alive and present. |
| Criterion 8: Inappropriate, Intense Anger or Difficulty Controlling Anger |
| Do you experience intense anger that feels disproportionate to the situation? Do you have difficulty controlling your anger, or do you experience frequent angry outbursts, fights, or recurrent physical confrontations? |
| Anger in BPD is often described as coming on suddenly and at an intensity that feels overwhelming and difficult to modulate. It may be triggered by perceived abandonment, criticism, or perceived injustice, and may feel entirely justified in the moment while producing significant regret afterward. The anger can be expressed or suppressed, but its intensity and the difficulty of regulating it are characteristic. This is one of the symptoms most frequently misunderstood as deliberate manipulation by others, when in reality the person is experiencing genuine emotional dysregulation that they are struggling to manage. |
| Criterion 9: Transient, Stress-Related Paranoid Ideation or Severe Dissociative Symptoms |
| Do you experience paranoid thoughts or feelings of unreality, depersonalization, or dissociation that tend to occur during periods of stress? |
| This criterion refers to transient experiences of paranoia or dissociation that are stress-related rather than persistent psychotic symptoms. During high-stress situations, particularly in interpersonal contexts, a person may begin to feel that others have hostile intentions, may feel detached from their own body or surroundings, or may experience the world as strange or unreal. These experiences typically resolve when the stress passes. They can be frightening and disorienting, and they are often more severe in the context of trauma history. |
Part 3: Understanding Your Self-Reflection
Now that you have read through the nine criteria, take a moment to reflect honestly. The clinical threshold for a BPD diagnosis is five or more criteria that are persistent, pervasive, and present across different relationships and contexts since early adulthood.
| What Your Reflection May Suggest | What to Do Next |
| You recognize 1 to 2 patterns strongly | These patterns may reflect normal human experiences, situational stress, or other conditions. Worth monitoring and discussing with a professional if they are causing significant distress. |
| You recognize 3 to 4 patterns consistently | You may be experiencing significant emotion dysregulation that deserves professional attention, whether or not BPD is the most accurate diagnosis. A clinical assessment is strongly recommended. |
| You recognize 5 or more patterns persistently and across contexts | This level of recognition warrants a formal clinical assessment for BPD. Please reach out to a mental health professional. You are not alone in this, and effective treatment exists. |
| Critical Reminder | This self-reflection exercise cannot diagnose BPD. Only a licensed mental health professional conducting a clinical assessment can do that. The purpose of this guide is to help you identify patterns that are worth discussing with a professional, not to provide a diagnosis. |
Part 4: The Four Types of BPD
BPD does not look the same in every person. Clinicians have described four presentations that represent different ways the core features of BPD can manifest. These are not official DSM-5 subtypes but are widely used in clinical understanding.
| Discouraged BPD | Quiet BPD or High-Functioning BPD |
| People with this presentation appear to function well externally. They tend to internalize their distress rather than directing it outward. Their fear of abandonment may cause them to cling to relationships silently rather than making demands. Their self-harm and suicidal behavior may be hidden. They may present as compliant, agreeable, and low-maintenance while experiencing profound internal distress. Key signs: Internal suffering, people-pleasing, hidden self-harm, collapse inward rather than outward, intense shame |
| Impulsive BPD | Charismatic or Thrill-Seeking BPD |
| The impulsivity criterion is the most dominant feature. People with this presentation may be charming, energetic, and exciting, with a tendency toward risk-taking behaviors, reckless decisions, and intense interpersonal engagement. They may struggle to sustain long-term commitments and may have histories of dramatic relationship endings and new beginnings. Key signs: Charisma combined with recklessness, difficulty sustaining commitments, excitement-seeking, impulsive decisions across multiple domains |
| Petulant BPD | Volatile or Unpredictable BPD |
| This presentation is characterized by alternating between emotional outbursts and withdrawal. The person may be easily frustrated, resentful, and stubborn, and may feel fundamentally misunderstood and unappreciated. Relationships are marked by intense conflict, with expressions of need that can feel demanding followed by withdrawal and push-pull dynamics. Key signs: Unpredictability, stubbornness, frustration, resentment, oscillation between needing and pushing away |
| Self-Destructive BPD | Masochistic or Self-Punishing BPD |
| Self-destructive behavior is the dominant feature. The person may engage in behaviors that are self-defeating or harmful, and may feel a strong sense of shame and self-hatred. They may sabotage relationships and opportunities that are going well. Self-harm is often a significant feature. There is frequently a profound internal critic and a tendency to feel fundamentally unlovable or worthless. Key signs: Self-sabotage, shame, self-hatred, self-harm, feeling fundamentally unworthy, sabotaging good things |
Part 5: BPD vs Other Conditions — The Most Common Confusions
BPD is one of the most frequently misdiagnosed conditions in mental health. People with BPD are often diagnosed with depression, bipolar disorder, ADHD, or anxiety disorders before BPD is identified, sometimes spending years in treatment that is not optimally matched to what they are actually experiencing. Understanding the distinctions matters.
BPD vs Bipolar Disorder
This is the single most common diagnostic confusion, and it is clinically consequential because the treatments are different. The key distinctions are:
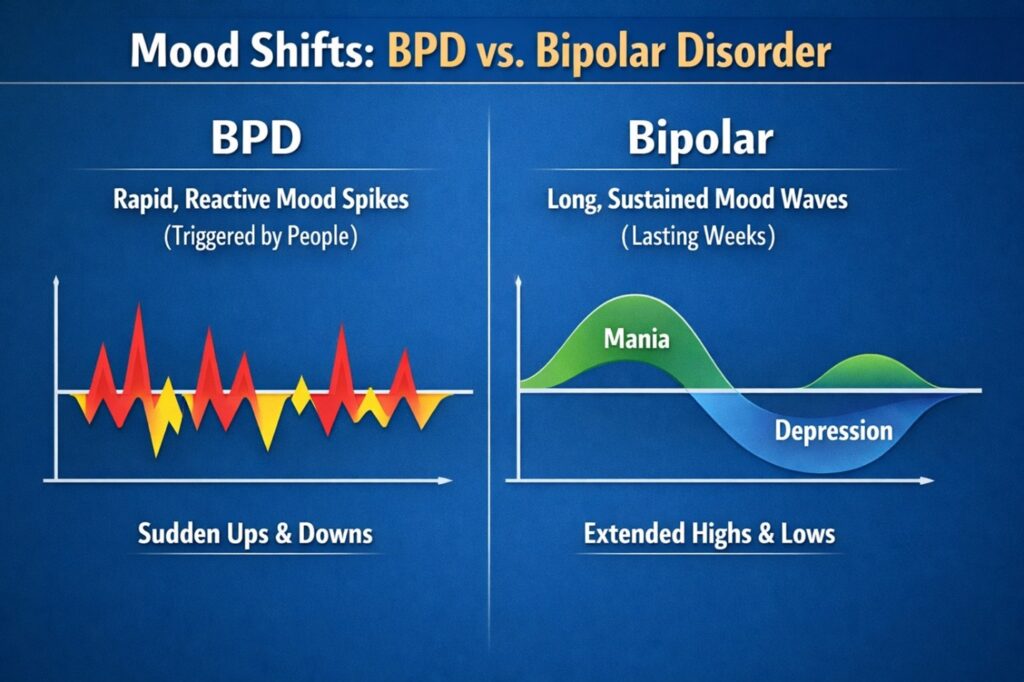
| BPD Mood Features | Bipolar Disorder Mood Features |
| Mood shifts last hours, rarely more than a few days | Mood episodes last days, weeks, or months |
| Mood shifts triggered by interpersonal events | Mood episodes often arise without clear external trigger |
| Rapid return to baseline once trigger resolves | Mood states are sustained regardless of circumstances |
| Identity instability and chronic emptiness present | Identity and sense of self more stable between episodes |
| Fear of abandonment and relationship instability central | Relationships affected by mood episodes but not identity-driven |
| DBT is first-line treatment | Mood stabilizers and specific psychotherapy are first-line |
It is also worth noting that BPD and bipolar disorder can co-occur. The presence of one does not exclude the other, and accurate differential diagnosis requires a thorough clinical assessment.
BPD vs PTSD and Complex PTSD
The overlap between BPD and PTSD, particularly Complex PTSD, is significant. Both involve emotional dysregulation, identity disturbance, interpersonal difficulties, and impulsivity. There is ongoing clinical debate about the relationship between the two, with some researchers arguing that much of what is diagnosed as BPD is better understood as Complex PTSD in people with childhood trauma histories.
From a treatment perspective, the distinction matters in terms of sequencing: DBT Stage 1 skills are foundational for both presentations, and trauma processing in Stage 2 is relevant when complex trauma is a significant part of the picture. An experienced clinician will assess both possibilities and tailor treatment accordingly.
BPD vs Depression
Depression and BPD frequently co-occur, and both involve emotional pain, emptiness, and loss of function. The key distinguishing feature is that BPD depression is typically reactive and episodic, closely linked to interpersonal events, while major depression is more sustained and pervasive. The identity disturbance, impulsivity, fear of abandonment, and relational instability that characterize BPD are not primary features of major depression without BPD.
BPD vs Narcissistic Personality Disorder
Both conditions involve relationship difficulties and emotional instability, but the underlying dynamics are different. In BPD, the core fear is abandonment and the core experience is emptiness and pain. In NPD, the core dynamic involves grandiosity and difficulty tolerating perceived insult to self-esteem. The two can co-occur, but they are clinically distinct and respond to different treatment approaches.
Part 6: Who Gets Diagnosed with BPD and the Problem of Gender Bias
Historically, BPD has been diagnosed significantly more often in women than in men, with some studies suggesting ratios of three to one or higher. This disparity has increasingly been recognized as reflecting diagnostic bias rather than actual prevalence differences.
Research suggests that men with BPD are more likely to be diagnosed with antisocial personality disorder, substance use disorders, or intermittent explosive disorder rather than BPD, because the same underlying emotional dysregulation tends to manifest in more outwardly directed behavior in men and more inwardly directed behavior in women, and the diagnostic system has historically been more attentive to inward presentations.
This means that many men with BPD go undiagnosed or are treated for conditions that address symptoms but not the underlying disorder. It also means that some women may be diagnosed with BPD when another diagnosis would be more accurate.
Regardless of gender, what matters is accurate assessment by a clinician who is aware of these biases and who conducts a thorough, individualized evaluation rather than applying pattern matching.
BPD in Adolescents
The DSM-5 notes that personality disorder diagnoses can be given in adolescents when features are pervasive and persistent. BPD specifically is often identified in adolescence, though some clinicians prefer to defer formal diagnosis until early adulthood to allow for developmental change.
Adolescents with emerging BPD features often present with self-harm, intense relationship difficulties, identity confusion, and significant emotional reactivity. Early identification and early DBT intervention is associated with better outcomes than waiting for the full disorder to consolidate in adulthood.
Part 7: BPD and Trauma — The Connection That Changes Everything
BPD and trauma have a relationship that is well-documented and clinically important. Research consistently shows elevated rates of childhood trauma, including emotional neglect, physical abuse, sexual abuse, and exposure to domestic violence, among people diagnosed with BPD. Some studies report that 70 to 90 percent of people with BPD have experienced significant childhood trauma.
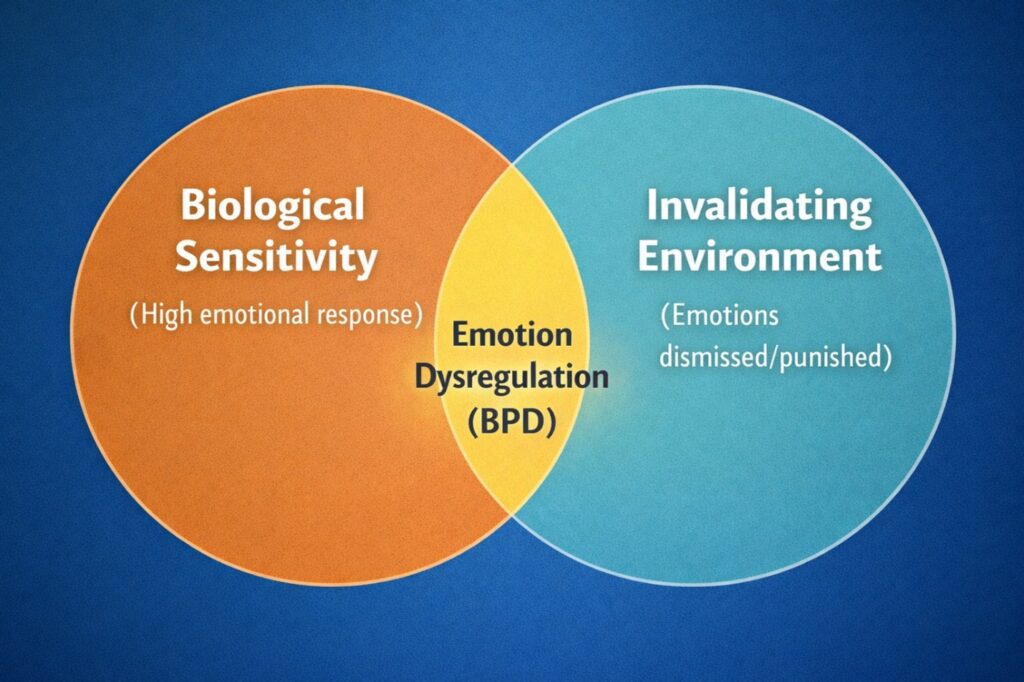
Marsha Linehan’s biosocial theory of BPD, which underpins DBT, proposes that BPD develops through the interaction of a biologically sensitive temperament with an invalidating environment. The invalidating environment is one in which the child’s emotional experiences are consistently dismissed, punished, trivialized, or ignored.
This theory does not locate the cause of BPD solely in trauma or solely in biology. It is a transaction: certain children are born with nervous systems that are more emotionally sensitive and reactive, and when those children grow up in environments that do not help them learn to regulate that sensitivity, the result is the pervasive emotion dysregulation that characterizes BPD.
This framing is deeply important for reducing shame. BPD is not the result of something inherently wrong with the person. It is the result of a sensitive system that did not receive the regulation support it needed.
| Kelly’s Perspective | In my clinical work, understanding the trauma and developmental history behind BPD changes the entire nature of the therapeutic relationship. When I understand that a client’s most difficult behaviors were originally adaptive responses to genuinely difficult circumstances, I can hold them with genuine compassion alongside the directness that DBT requires. The two are not in contradiction. |
Part 8: How BPD Is Formally Diagnosed
A BPD diagnosis is made by a licensed mental health professional through clinical interview and assessment. There is no blood test, brain scan, or questionnaire that can diagnose BPD. The diagnosis requires clinical judgment applied to a thorough assessment.
The Diagnostic Process
- Comprehensive clinical interview covering current symptoms, life history, and functional impairment
- Assessment of all nine DSM-5 criteria, including how long they have been present and how pervasive they are across different contexts
- Ruling out medical conditions that can mimic BPD symptoms, including thyroid disorders and neurological conditions
- Differential diagnosis to distinguish BPD from other conditions with overlapping presentations
- Assessment of co-occurring conditions, which are the rule rather than the exception in BPD
A BPD diagnosis can be given after one thorough assessment or may require several sessions. Some clinicians use validated screening tools such as the McLean Screening Instrument for BPD or the Zanarini Rating Scale for BPD as part of their assessment. These tools are not diagnostic on their own but can provide useful structured information.
Why BPD Is Often Missed
BPD is missed for several reasons. Clinicians who are not specifically trained in personality disorder assessment may not systematically assess the nine criteria. BPD frequently co-occurs with depression or anxiety, and the more visible presenting symptoms can capture the diagnostic attention while the underlying BPD goes unrecognized. The stigma around BPD within some clinical communities can lead some providers to avoid the diagnosis. And as discussed, gender bias affects who gets assessed for it.
If you believe you may have BPD and have not received an adequate assessment, it is entirely appropriate to ask a clinician directly about whether BPD has been considered and how it has been assessed.
Part 9: DBT and BPD — Why This Treatment Is the Gold Standard
Dialectical Behavior Therapy was developed by Marsha Linehan specifically to treat BPD. Before DBT, people with BPD were considered among the most difficult to treat in mental health, with high rates of treatment dropout, clinician burnout, and chronic suicidality.
DBT changed that picture entirely. Randomized controlled trials have demonstrated that comprehensive DBT reduces suicidal and self-harming behavior, decreases psychiatric hospitalizations, reduces treatment dropout, and improves overall functioning in people with BPD. It is now recognized as the first-line, most evidence-supported treatment for BPD by major clinical organizations worldwide.
Why DBT Works for BPD
DBT works for BPD because it was built on the biosocial theory that explains BPD. It directly addresses the emotion dysregulation at the core of the condition through four skill modules:
- Mindfulness teaches the observational awareness that allows the person to create a moment of choice between emotional stimulus and behavioral response. This is foundational because BPD involves collapsing the gap between feeling and acting.
- Distress tolerance provides tools for surviving crisis moments without making things worse. Given the high-intensity crisis states that are characteristic of BPD, having a practiced set of tools for surviving rather than reacting is transformative.
- Emotion regulation teaches clients to understand, name, and modify emotional responses. The specific combination of high sensitivity and poor regulation that characterizes BPD is directly targeted here.
- Interpersonal effectiveness addresses the relational instability, fear of abandonment, and communication difficulties that characterize BPD in ways that generic communication skills training does not reach.
Beyond the skills, DBT’s dialectical philosophy, the simultaneous holding of acceptance and change, is particularly suited to BPD. The radical acceptance that is foundational to DBT directly addresses the invalidation that contributed to BPD’s development. And the therapeutic relationship in DBT, which is explicit, boundaried, warm, and skills-focused, provides a reparative relational experience for clients whose early relational experiences were damaging.
What Board Certification Means for BPD Treatment
Not all therapists who say they practice DBT are providing the comprehensive, adherent DBT that the research supports. The DBT-Linehan Board of Certification, Certified Clinician designation indicates that a clinician has met rigorous training, supervision, and assessment standards established by the organization founded by Marsha Linehan herself.
For someone with BPD, who may have already experienced years of treatment that did not work, working with a board-certified DBT clinician provides the highest reasonable assurance that the treatment being delivered reflects the evidence-based model.
Part 10: Recovery from BPD — What the Evidence Actually Shows
One of the most harmful myths about BPD is that it is untreatable or that people do not recover. The evidence directly contradicts this.
Longitudinal research, including the McLean Study of Adult Development which followed people with BPD over ten years, found that approximately 85 percent of people with BPD achieved symptom remission at some point during the study period. The NIMH-funded Collaborative Longitudinal Personality Disorders Study found similar outcomes. These are not studies of people who received ideal treatment. They are naturalistic studies of how BPD actually unfolds over time.
With comprehensive, evidence-based treatment such as DBT, outcomes are significantly better than natural course alone. Studies have consistently shown that people who complete DBT treatment experience reductions in self-harm, suicidality, impulsivity, and emotional instability that are clinically significant and durable.
What Recovery Looks Like
Recovery from BPD does not mean the complete elimination of all emotional sensitivity. It means developing enough regulatory capacity that emotional experience no longer drives the behaviors and relationship patterns that cause harm. It means having a more stable sense of who you are. It means relationships that can hold conflict without shattering.
Many people who have recovered from BPD describe a profound appreciation for their emotional sensitivity alongside an entirely different relationship to it. The intensity that was once a source of destruction becomes, with skill, a source of depth, connection, and aliveness.
| From Our Clients at Southside DBT | Kelly’s DBT program, and expertise has taught me crucial skills that I have needed my whole life. In the last three years I have experienced tremendous growth. I can communicate more effectively. I am learning to face tough situations without giving up. I have learned to feel emotions that I thought were impossible to feel. |
Part 11: What to Do Next
If this guide has resonated with you, the most important thing you can do is reach out for a professional assessment. Not a quiz. Not a checklist. A real, thorough clinical evaluation by a licensed mental health professional with experience in personality disorders.
When seeking assessment or treatment, ask specifically whether the clinician has experience with BPD, whether they practice comprehensive DBT or another evidence-based approach, and whether they have specific training in personality disorder assessment. For those seeking DBT specifically, asking whether the clinician holds the DBT-Linehan Board of Certification is the highest standard of verification available.
Receiving a BPD diagnosis can feel devastating, validating, frightening, or relieving, sometimes all at once. Whatever you feel, what matters is what comes next. And what comes next, with the right treatment, is the possibility of a life that is genuinely different from the one that brought you to this guide.
| Seeking BPD Assessment or DBT Treatment in Georgia? Southside DBT specializes in comprehensive, board-certified DBT treatment for BPD and emotion dysregulation. Kelly Pinnick | DBT-Linehan Board of Certification, Certified Clinician | Telehealth across Georgia (770) 880-2538 | kelly@southsidedbt.com Accepting: Aetna | Anthem BCBS GA | Cigna | United Healthcare | Self-Pay $150/session |
Crisis Resources: 988 Suicide and Crisis Lifeline: Call or Text 988 | Crisis Text Line: Text HELLO to 741741